D+18: Bolus

No, not when you know as much about house repair as I do. But it does mean a lot more work than I had planned (this was a painting project, recall).
Later in the day I will blog up my meeting with the neurologist, detailing the objectives, timetables, and jumping-off points of Operation Bolus.
Remember the 100-yard dash metric? That one didn't prove so useful. I tried it about at one week, and again one month, after my diagnosis, and I wound up giving myself a cramp that hurt by leg muscles. So I stopped. But now that I am even more disabled (yes, I have used that term a couple of times to describe myself), I had this hunch that my 'running' would be so impaired that I was not likely to pull any muscles. Fortunately, I was right.
Both times, I pointed skywards with both index fingers, Like Joe Montana used to do after a nice touchdown pass. Only, my left index finger doesn't straighten, so it was kind of a hook and point gesture. There were high school boys in the next field, warming up for baseball. They're hale, fit, healthy, and destined for lives of alcohol dependancy, taxation, television, and surly children.
Mission accomplished.
I walked home, past a teenager with bandana low over his eyebrows. He was shooting baskets, and this is the thing about basketball, no matter what barriers of race, age, or social category separate you, on the court, any basketball player will accept any other. Except if you're a woman, in which case you gotta carry a little bit more ganas. But I know several women, (my lovely wife among them), who have no problem taking to the court and baffling teenage boys. I have video to prove it.
So as I walked past, I asked him if I could shoot one. He passed me the ball, which I fumbled, and did that skip-run trying to retrieve before it hit a car. I fumbled it some more after I recovered it. "I used to play all the time," I said, putting it in terms I thought he would understand, "until I messed up my leg." I put in a close backboard shot and was grateful it went in, as I have a notable tendency to miss from any distance.
On the way home I crossed with a blind woman using a seeing-eye dog. That's something I didn't even consider putting on the table during the Amputation Derby. I think neither she nor I would want to trade. However, if I were progressing faster, as some of my fellows PWALS are, I'd probably leap at the chance. And I don't want to sound smug, talking about my 'sprint.' It's just that I have been given to pilot this one body, and this one life. So I have to treat it on its own terms, and often that means its frame of reference becomes the only frame of reference.
My technical copy of Mitsumoto's "Amyotrophic Lateral Sclerosis" arrived yesterday. Good.
Operation Bolus
I went to see the local neurologist yesterday. I really like this guy. We planned Operation Bolus. This operation is based on the intelligence that penicillin, the father Abraham of beta-Lactam antibiotics, was examined in the Rothstein study, along with ceftriaxone, and was found to be effective in increasing expression of GLT-1, which clears out the used glutamate which is thought to kill the motor neurons. But, as Rothstein notes, penicillin has trouble crossing the blood-brain barrier.
And, as you know from following Dee Chiplock's story, ceftriaxone is expensive. And as you can intuit from the press release there is a pretty penny to be made if the human trials show that ceftriaxone is effective against ALS. The patent claims have already been staked:
The newfound ability of ceftriaxone, other beta-lactam antibiotics, and other classes of drugs to activate glutamate transporters and to protect nerves, and the drugs' potential therapeutic use in a wide range of neurological and psychiatric conditions, are covered by patent applications held by The Johns Hopkins University and licensed to Ruxton Pharmaceuticals, Inc.
Yet, as my doctor noted, penicillin, if given in large enough doses, does cross the blood-brain barrier.
The case in point apparently is the disease syphilis which attacks the brain, and in which (forgive me if I misunderstood), even advanced cases can be treated by large doses of penicillin. This means that an effective dose does reach the brain.
And, as I noted, it's passed out of patent now. Nobody owns it. My doctor says it is "as cheap as water."
I doubt that the patent, if granted, would preclude doctors from treating their patients with penicillin for ALS. If it did, 30,000 people would get acne over night. Penicillin can be used to treat pimples. I have a prescription right here to prove it. He gave "folliculitis" as the reason. And in fact, I do have a big pimple on my cheek. Indeed, I have noticed more than one in the past few weeks. It's a severe problem that worries me to death, and so I'm glad my neurologist is on top of things!
I have no objection to a brilliant researcher like Rothstein making money from his excellent discoveries. The American pharmaceutical and health delivery systems are deeply unjust, and need to be changed, but a way must be found to reward someone like Rothstein.
That said, I wouldn't mind a cheaper way to excite my expression of GLT-1.
So in Operation Bolus, I will start taking large doses of penicillin, one gram twice a day. The objective is to maintain my inhale volume, grip strengths, and one-legged balance durations at current levels. The timetable is to begin some time in early March, and continue the operational tempo indefinitely -- 20 days or more. The jumping off point -- and here is the best part -- is my mouth. Yes, I'm going to take oral penicillin. No needles!
"Bolus" means, in this case, a big pill. I'm sure the pill will be reasonably sized, so I guess it's meant to convey the concept of the dose being hefty.
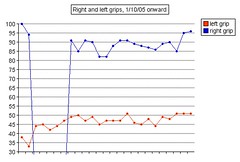
I think it is time to analyze the results of the Ceftriaxone. It's now 18 days after the final dose, and I would have expected to see a downward trend by this point. The study mentions positive effects that "persisted for at least seven days in vitro." That language is ambiguous enough to allow for indefinite benefit, but I take it to mean that seven days is about all you can confidently expect. And while there is plenty of bouncing around in my metrics data, I am surprised that left and right grips are both at record highs. Touch wood, we seem to be in a plateau right now. I credit my slow-mover history as the reason I have not yet seen a decline in the post-ceftriaxone metrics. Maybe I have somewhat good GLT-1 expression, for an ALS patient, and my system is almost keeping up, at the moment. Maybe, maybe, maybe. Who knows? I mentioned to the doctor that as a systems debugger, I have half a mind to deprive the subject of treatment until we can see the data change. He shook his head and told me that you don't want to mess around when your life is at risk. I agree. Who cares if I don't get good data, as long as I'm around to complain about it!
We're holding the ceftriaxone in reserve and will commit the reserve if opposition forces threaten a breakout. There are rumors they'll land at Normandy, but we are convinced that their real objective is Le Havre or ports to the East.
I have mentioned before that I often think of my struggle against ALS in terms of a war (when I'm not thinking of it in terms of computer programming), and I am a student of World War Two history, and that, unfortunately, means being the Germans, because I am on the defensive. I don't like being the Germans, I'd rather be the Americans. And I hope the day will come when we go on the offensive against ALS. And then I'll switch sides, and be the Americans.
posted by brainhell at 5:59 AM
![]()

<< Home