D+2: Riluzole reaction
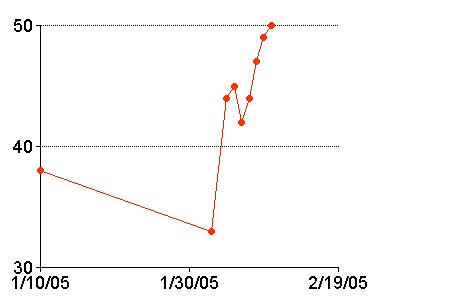
Here is the left grip strength chart so far. Today my left grip strength is at 50 pounds (ALife: 50.5, 47, 48). Compared to 33 pounds (2/2/05), that's 51 percent stronger. Compared to 38 (1/10/05) pounds, that's 31 percent stronger. Do I feel stronger in my hands? No. But I do feel stronger and better overall. However, I think this is a mind-body response to the good news.
But the breathing is back down to 4600 from yesterday's 4750, though I'll try again after breakfast has cleared out a bit more.
A very strong and athletic wind-surfer we know, who is about my age and who gets exercise all the time, has a left grip of 115 and a right grip of 116. This symmetry is a feature, I think, of people who are in good shape. My wife, who is strong, healthy, thin1 and beautiful, and who competed in college sports, has nearly equal strength in left and right hands too.
Oh, my right hand fell asleep again last night, in that really mild way I have tried to describe. The reason why neither arm did so during the period of the infusions is rather evident, when you think about it: I was much more conscious of my arm positions, even when sleeping, because I did not want to disturb the IV in my arm. It had an effect on how I slept2.
I am the king of rash (but correct!) decisions, and this morning I can't make myself take the riluzole. I have been reading about the possible liver damage, and just between you and me, I don't think it has shown any benefit beyond the three-month extension of the initial trial.
Over a year ago when I was diagnosed, my clinic doctor said: "what we're now seeing, in Ireland and in Britain and in other registries where people are starting the drug earlier, that there's a substantial benefit from the drug. It's very safe, but it is very expensive."
Well, I don't think it's "very safe," and in the past year I didn't heard a peep about that "substantial benefit."
This morning I sent an email and left a voicemail for the patient contact at the ALS clinic, asking for updated data on the ongoing effects of riluzole.
Glutamate is a necessary compound; your body cannot function without it. Normal bodies clear out the glutamate and replace it with new stuff. In the case of ALS, glutamate is not cleared out as much as it should be, and it builds up, damaging the motor neurons. Riluzole suppresses glutamate throughout your whole body. Which, if I may say so, seems kind of stupid. That's like applying a tourniquet to the neck to protect the body from harmful oxidation.
So, in my view, it's a poison, and it doesn't do much for ALS. I can't make myself take it, no, not even until I talk to the experts. I will, however, tell the experts about my decision, and if they can convince me to get back on it, then I will. Or if my metrics take a complete dive, I will.
You might think that that ceftriaxone has made me overconfident. Well, maybe so. But I don't count on the ceftriaxone to save me. I think it is possible that next time I use the ceftriaxone, the benefit will be somewhat less dramatic than it was this time. And so on, and so on, until it has almost no effect. I could be wrong about that, and I hope I am, but I am emotionally prepared for the possibility.
Anyway, nuts to the riluzole. For now.
The "D+[n]" notation in the post header tracks how many days is has been since my last dose of ceftriaxone. The 1/6/05 piece in Nature said that the beneficial effects last a substantial time after dosing (at least seven days in vitro (test tube) and four to 6 weeks in live rodents). The "D+[n]" notation is my way of reminding myself to track the changes.
_____________
1
No, I don't think thin is better. I just threw that in to infuriate people who are obsessed with thinness.
2
Neither 'affected' nor 'effected' is appropriate here. We should all just learn that there is no such word as the one we are groping for. This space is empty.
posted by brainhell at 7:30 AM
![]()

<< Home